Introduction
Food-drug interactions (FDIs) represent a significant clinical concern that can substantially alter the pharmacokinetic and pharmacodynamic properties of medications, potentially leading to therapeutic failure or adverse drug reactions. The interaction between food and medications occurs through various mechanisms including changes in drug absorption, metabolism, distribution, and elimination. Understanding and recognizing these interactions is crucial for healthcare professionals to ensure optimal therapeutic outcomes and patient safety.
The prevalence and clinical impact of food-drug interactions have been extensively documented in pharmaceutical literature. Studies have demonstrated that food can significantly alter the bioavailability of numerous medications through multiple mechanisms [1].
Food-drug interactions can be classified into two main categories: pharmacokinetic interactions, which affect drug absorption, distribution, metabolism, and excretion; and pharmacodynamic interactions, which modify the drug's mechanism of action or its effects on target organs. The pharmacokinetic interactions are more commonly observed and clinically significant, particularly affecting drugs with narrow therapeutic indices such as anticoagulants, immunosuppressant, and certain cardiovascular medications [2].
A study revealed significant knowledge gaps regarding food-drug interactions, with only 54% of respondents demonstrating adequate knowledge. Similarly, in another research, among healthcare professionals in India found that while 78% of participants were aware of the existence of food-drug interactions, detailed knowledge about specific interactions was limited [3,4].
Nurses, who often serve as the first point of contact with patients, play a pivotal role in identifying and preventing potential food-drug interactions. However, study demonstrated that nursing staff frequently lack comprehensive knowledge about food-drug interactions, with knowledge scores varying significantly based on years of experience and educational background. This knowledge deficit is particularly concerning given that nurses are often responsible for medication administration and patient education regarding proper medication use [5].
The management of food-drug interactions requires a multidisciplinary approach involving physicians, pharmacists, nurses, and other healthcare professionals. Pharmacists, with their specialized training in pharmacology and therapeutics, are uniquely positioned to identify, prevent, and manage food-drug interactions [6,7].
Several barriers impede the effective implementation of food-drug interaction knowledge in clinical practice. Time constraints, heavy workload, and lack of accessible resources are commonly cited obstacles. Healthcare professionals often lack confidence in counseling patients about food-drug interactions due to insufficient training and limited access to comprehensive, up-to-date information resources [8].
Communication gaps between different healthcare professionals and between healthcare providers and patients further complicate the management of food-drug interactions. The development and implementation of standardized protocols and checklists can help ensure consistent patient education and monitoring [9].
The assessment of food-drug interaction knowledge among healthcare professionals serves multiple purposes, including identifying knowledge gaps, evaluating educational interventions, and informing curriculum development.
Aims and Objective
To explore the awareness on FDIs among the health care professionals who are in first contact with the patients through a questionnaire.
To analyze the experience of FDI among the health care professionals in their practice.
To analyze the suggestions on ‘’how to improve the awareness & reporting practice on FDI” among the health care professionals and patients.
Methodology
After getting Institutional Ethics committee approval, this questionnaire based cross sectional study was conducted among the Nurses, CRRIs, Postgraduates, Registered medical practioners with their voluntary informed consent (N=350). There were 3 yes or no type questions and 15 multiple choice questions and 2 open ended questions. Data from the study was analyzed using suitable statistical method.
Results
The present study assessed Food-Drug Interaction (FDI) knowledge, awareness, and perceptions of 350 healthcare professionals comprising faculty (7.7%), post-graduates (10.6%), interns (16.3%), and nurses (65.4%). The findings reveal a concerning knowledge-attitude-practice gap that has significant implications for patient safety and medication management.
Several areas demonstrated satisfactory knowledge levels among study participants. The high awareness (92%) regarding thyroid hormone administration timing reflects the emphasis placed on this interaction in clinical practice and patient counseling. Knowledge regarding prednisolone and dietary sodium restriction (86% correct) and the interaction between H1 antihistamines and alcohol (59% correct) was also relatively good. These findings suggest that when food-drug interactions are frequently encountered and consistently emphasized in clinical practice, healthcare professionals develop better awareness and retention. The moderate awareness (58%) regarding Tetracycline and Fluoroquinolone interactions with calcium-containing products indicates room for improvement but suggests baseline understanding exists.
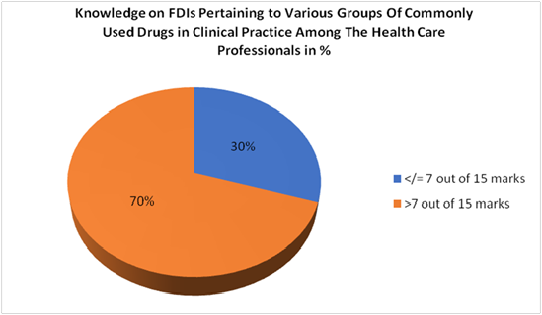
15 knowledge based questions addressing the known FDIs of various groups of commonly used drugs in clinical practice. Total analysis was done out of 15 marks and results were expressed in percentage as score >7 and < 7 out of 15 knowledge based questions on FDIs
| Questions on FDIs Pertaining to Various Groups of commonly used Drugs in Clinical Practice | Correct response n (%) | Incorrectresponsen(%) | Mean+SD | |
| 1. | FDI definition | 290 (82%) | 60 (17%) | 0.83+0.38 |
| 2. | Consumption of which food helps to minimize the risk of fluid retention while consuming Prednisolone? | 302 (86%) | 48 (13%) | 0.49+0.50 |
| 3. | Which of the following beverages is not recommended with H1 antihistamine? | 208 (59%) | 142 (40%) | 0.77+0.42 |
| 4. | Food that does not affect the efficacy of Proton pump inhibitors is? | 208 (59%) | 142 (40%) | 0.86+0.35 |
| 5. | Iron supplements absorption is reduced by all except | 185 (52%) | 165 (47%) | 0.59+0.49 |
| 6. | Drugs with NSAIDS and ASTHMA medications should not be consumed with… | 227 (64%) | 123 (35%) | 0.59+0.49 |
| 7. | When do Thyroid hormone tablets should be consumed? | 324 (92%) | 26 (7%) | 0.53 +0.50 |
| 8. | Drugs like Albendazole, Antifungal medications should be consumed which kind of food to increase their absorption? | 193 (55%) | 157 (44%) | 0.65 +0.48 |
| 9. | Food that increases the absorption of Statins higher than the normal level resulting in greater risk of side effects | 163 (46%) | 187 (53%) | 0.93+0.27 |
| 10. | Ant diabetic drugs like Acarbose, Voglibose, when it should be taken? | 107 (30%) | 243 (69%) | 0.55+0.50 |
| 11. | Patients on Heparin /Warfarin should avoid consuming foods to prevent complication? | 84 (24%) | 266 (76%) | 0.47+0.50 |
| 12. | Antibiotics like Tetracycline, Fluoroquinolones should not be consumed with? | 203 (58%) | 147 (42%) | 0.31+0.46 |
| 13. | When taking ACE inhibitors like Captopril avoid consuming potassium rich food like? | 133 (38%) | 217 (62%) | 0.24+0.43 |
| 14. | Which age group do you think of having greater risk for FDI? | 156 (44%) | 17 (4%) | 0.58 +0.49 |
| 15. | Which organ is more likely to be affected when allopathic and ayurvedic medicines interact with each other? | 236 (67%) | 33 (9%) | 0.38 +0.49 |
| H-Statistic | p-value |
| 26.3161 | 0.000002 |
Interpretation: There is a statistically significant difference in scores between the three groups (p < 0.001).
| Comparison | U-Statistic | p-value |
| FACULTY vs PG | 603.50 | 0.350401 |
| FACULTY vs CRRI | 1350.00 | < 0.001 |
| PG vs CRRI | 1539.50 | 0.000922 |
Bonferroni-adjusted significance level: α = 0.0167
Discussion
The present study assessed Food-Drug Interaction (FDI) knowledge, awareness, and perceptions of 350 healthcare professionals comprising faculty (7.7%), post-graduates (10.6%), interns (16.3%), and nurses (65.4%). There were 3 yes or no type questions and 15 multiple choice questions and 2 open ended questions with the reliability score of Cronbach’s alpha 0.8 which was statistically significant.
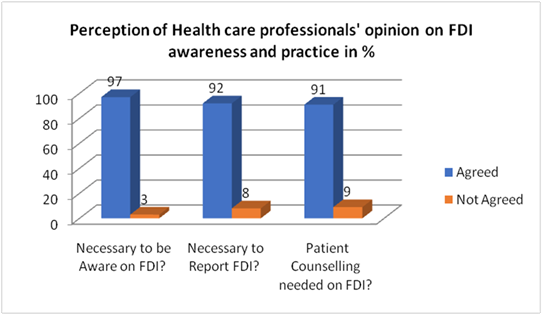
While healthcare professionals demonstrated near-universal recognition of FDI importance—with 97% agreeing that FDI awareness is necessary, 92% endorsing the need to report FDIs, and 91% supporting patient counselingactual knowledge performance was substantially lower (Figure 1). Regarding the total scores on FDIs knowledge, 70% of participants achieved good knowledge scores (>7/15 marks), with 30% scoring at average or poor levels (Figure 2,3). This pattern of high awareness coupled with moderate knowledge parallels findings from Ethiopia, where healthcare providers demonstrated 89% knowledge and 82% positive attitude, yet exhibited poor practice at only 60% [10].
The highest knowledge scores were observed for thyroid hormone administration timing, with 92% of healthcare professionals correctly identifying that thyroid medications should be consumed on an empty stomach. Benvenga et al. demonstrated through rigorous pharmacokinetic studies that levothyroxine absorption is significantly impaired up to 55% when taken with food, particularly coffee, dairy products, and high-fiber foods [11] (Table 1).
The most alarming finding of this study was the critically low awareness regarding food interactions with anticoagulant therapy (Heparin/Warfarin), with only 24% of healthcare professionals providing correct responses.Many studies emphasized that patients inadequately counseled about dietary consistency may experience dangerous variations in their INR, leading either to bleeding complications (if vitamin K intake decreases) or thromboembolic events (if vitamin K intake increases) [2,12] (Table 1).
Another critical knowledge deficit identified in this study pertains to antidiabetic medications, specifically alpha-glucosidase inhibitors (acarbose and voglibose), with only 30% of participants correctly identifying the optimal timing of administration. This finding is particularly significant because the mechanism of action is entirely dependent on proper timing relative to meals. Koziolek et al.revealed that alpha-glucosidase inhibitors must be taken with the first bite of food to effectively reduce postprandial blood glucose spikes by up to 30-40% [13] (Table 1).
The study revealed that only 38% of healthcare professionals correctly identified the interaction between ACE inhibitors (such as captopril) and potassium-rich foods. When patients consuming ACE inhibitors also have high dietary potassium intake from foods such as bananas, oranges, potatoes, tomatoes, spinach, and avocados, the additive effect can lead to dangerous elevations in serum potassium levels (Table 1).
Hyperkalemia is a potentially life-threatening condition that can cause cardiac arrhythmias, muscle weakness, and in severe cases, cardiac arrest. This is particularly concerning in populations with underlying renal impairment. Elderly patients are at particularly high risk for ACE inhibitor-related hyperkalemia due to age-related decline in renal function, polypharmacy, and frequent use of potassium-sparing diuretics or potassium supplements. The knowledge gap identified in our study therefore has particularly serious implications for geriatric patient populations [9,14].
Regarding tetracycline and fluoroquinolone interactions with calcium-containing products, 58% of participants provided correct responses. These interactions can reduce antibiotic absorption by up to 90%, potentially leading to therapeutic failure and development of antibiotic resistance. The moderate awareness level in our study suggests room for substantial improvement through targeted educational interventions. Similarly, 59% of participants correctly identified interactions related to H1 antihistamines with beverages (alcohol) and proton pump inhibitors with food. The interaction between antihistamines and alcohol can potentiate central nervous system depression, leading to excessive sedation, impaired cognitive function, and increased risk of falls and accidents (Table 1).
Our study findings closely align with Gnanavel et al. study showing high conceptual awareness (82%) but variable specific knowledge, suggesting that this represents a consistent pattern across Indian healthcare settings rather than an isolated institutional issue. The knowledge gaps identified in this study have direct implications for patient safety and therapeutic outcomes [4].
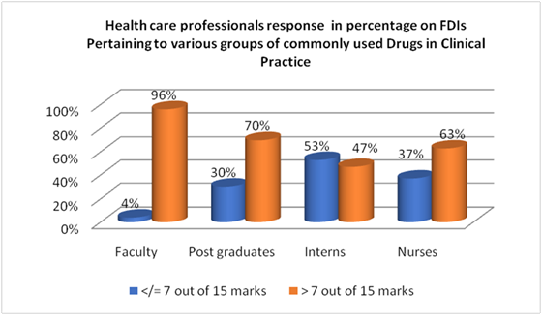
When compared the scores of Professors, Post graduate, and Interns using the Kruskal-Wallis test, revealed a statistically significant difference in scores between the three groups (H = 26.32, p < 0.001). The post-hoc pair wise comparisons also showed Highly significant difference (p < 0.001) between faculty vs Interns and Postgraduates vs Interns with (p = 0.001). The CRRI group demonstrates significantly lower median scores (7.0) compared to both FACULTY (9.0) and PG (9.0) groups. FACULTY and PG groups show similar performance levels with no statistically significant difference between them. Addressing this knowledge gaps among the primary health care professionals requires not only educational interventions but also systematic changes in clinical workflow, resource availability, and institutional support. Interprofessional education initiatives that bring together students and practitioners from different healthcare disciplines to learn about food-drug interactions collaboratively may help address the knowledge gaps identified in our study. Such initiatives can promote understanding of each profession's role in interaction management, facilitate communication and coordination, and ensure consistent patient education across the healthcare team. The variable knowledge levels observed among different healthcare professional categories in our study underscore the need for standardized, interprofessional educational approaches that ensure all team members possess core competencies in food-drug interaction recognition and management (Table 2,3).
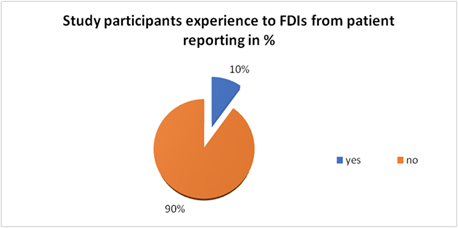
The 10% reporting rate of FDIs aligns with literature showing 70% of patients don't disclose dietary supplement use like Iron-calcium interactions which are well-documented (50-60% reduction in iron absorption) This represents a critical gap in pharmacovigilance and patient safety. Suggests most FDIs remain undetected in clinical practice. Hence Systematic dietary history-taking during medication reconciliation, Integration of FDI screening into electronic health records are needed to give quality in patient care and safety. (Figure 4).
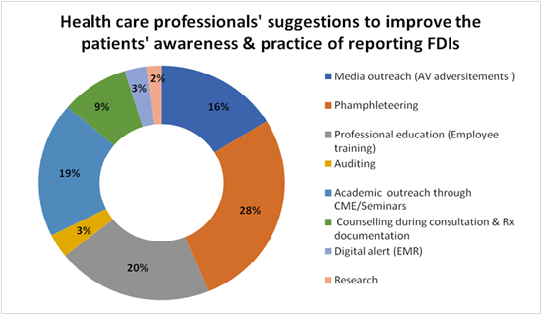
Healthcare professionals identified pamphleteering (28%) and professional education through employee training (20%) as the top two strategies for improving patient awareness and reporting practices of FDIs (Food-Drug Interactions) also highlighting the critical role of information dissemination in addressing this issue. Academic outreach through CME/Seminars (19%) and media outreach via audiovisual advertisements (16%) were also frequently recommended, emphasizing the importance of learning the FDI updates. Interestingly, technology-based solutions like digital alerts in EMR (3%) and periodic auditing (3%) suggest the other alternative approaches to enhance the FDI practice and patient safety. Overall, the results suggest a strong preference for proactive educational interventions over reactive monitoring systems in enhancing FDI reporting practices (Figure 5).
Conclusion
The findings underscore the urgent need for comprehensive, evidence-based educational interventions targeting frontline healthcare professionals who are in direct contact with patients. Given that nurses, Interns, and postgraduate students play pivotal roles in medication administration and patient counseling, ensuring their competence in identifying and managing food-drug interactions is paramount for patient safety and optimal therapeutic outcomes.
Based on the study findings, several recommendations are proposed to enhance food-drug interaction knowledge and practice among healthcare professionals:
Mandatory continuing education programs focusing on food-drug interactions should be implemented for all healthcare professionals, with particular emphasis on high-risk medications such as anticoagulants, antidiabetics, and cardiovascular drugs.
To include quick-reference guides, mobile applications, or integrated electronic health record systems that provide alerts and recommendations regarding food-drug interactions during medication ordering and administration.
Standardized protocols for patient counseling regarding food-drug interactions should be developed and implemented across healthcare institutions.
Multidisciplinary approach involving physicians, pharmacists, nurses, and dietitians should be fostered to comprehensively address food-drug interactions in patient care. Regular interprofessional case conferences and collaborative rounds can facilitate knowledge sharing and improve overall awareness.
Institutional quality improvement initiatives should include monitoring and reporting systems for food-drug interaction-related adverse events. Analysis of these incidents can help identify recurring problems and guide targeted educational interventions.
In conclusion, while this study identified important knowledge gaps in food-drug interaction awareness among healthcare professionals, it also provides a foundation for developing targeted educational interventions and practice improvements. Further longitudinal studies examining knowledge retention and the relationship between knowledge levels and clinical practice patterns would provide valuable insights for continuous quality improvement in medication safety.
Limitations
As a cross-sectional study conducted at a single tertiary care hospital, the findings may not be generalizable to other healthcare settings or geographic regions. The knowledge and awareness levels may vary based on institutional practices, educational programs, and patient populations.
The study did not assess the sources of knowledge or the effectiveness of different educational interventions, limiting our ability to recommend specific educational strategies. Future studies should employ longitudinal designs to assess knowledge retention over time and the impact of educational interventions on both knowledge levels and patient outcomes.
Declarations
Acknowledgement
We thank the department of pharmacology and all heath care professional for their volunteering to complete this study.
Conflict of Interest
NIL
Funding
Self- funding